Anyone arriving at the site will find that the records from 4 of the historical years have been presented in detail. These let you see the actual case materials on which we’ve based some of the conclusions we’ve drawn.
But we have 46 more years’ worth of historical records ready to be loaded. These might provide the basis for an MA or DPhil or PhD thesis. We can make the records for any of these years available to anyone interested to engage. The hope is that anyone doing so would try to replicate or develop what Margaret Harris has done for 1875, 1890, 1905 and 1920. This would involve curating the records for display and chasing historical detail on issues locally or globally linked to that year that the cases in these records prompt.
Our hope is to make this site of interest for visitors from Argentina to Japan by being intensely local. Our belief is that if people from anywhere in the world look closely at what happens in a particular area they will recognise commonalities between the experience there and their own.
This means that we hope anyone adopting a year or group of years will chase:
local North Wales details
local details from elsewhere that brings out common features between there and North Wales
details that add to our understanding of Mental Health and its disorders as well as general medicine and its disorders
In due course we will supplement what’s here with material that will be broadly labelled perhaps ‘1950’ telling the story of mental health in the period between the historical era and the contemporary era.
There will also be a further section, notionally termed 2001, which will give a picture of the patient flow through the Hergest Unit in North West Wales in that year and will help bring out the changing features between now and the historical period.
In terms of local detail the politics of healthcare in North Wales in recent decades has been fascinating and recapitulates the story that led to the founding of the North Wales Asylum in the first instance. The hope here is that bringing out aspects of the contemporary picture will enable people to better understand the factors that were at play in the historical period also – it will help humanise the historical period.
This is an active site. In addition to using the site to get a research degree, you can become part of the Madness as:
An informal researcher struck by some curiosity of healthcare or mental healthcare history that you feel would be of interest to others coming to this site
As someone interested in the historical period and keen to bring out social aspects of this that have impinged on healthcare either in the UK or anywhere else in the world
As someone from North Wales who has photographs or other artefacts that might help feed the imagination of people visiting the site.
As an artist stimulated to write a story, play or poem bearing on mental illness that could sit beside the stories from Dangerous Asylums already on the site.
As someone aware of stories, plays and poems bearing on mental illness.
As a musician or composer whose work has links to the themes of health and illness, particularly mental illness (see Night Terrors).
As someone aware of music that tells something of the experience of mental illness 100 years ago or today.
As a visual artist interested to contribute to the material that is here.
In all these cases we would love to hear from you. You can contact us on the details below:
The work that led to this website began in the early 1990s when the Department of History at Bangor University applied for a Wellcome Trust grant to investigate the history of the North Wales Asylum at Denbigh, sometimes called the Denbigh Asylum. The Wellcome Trust knocked the grant back. The world had too many asylum histories, it didn’t need another.
Merfyn Jones, then the Professor of History at Bangor, later Vice Chancellor of the University and Chair of Betsi Cadwaladr University Health Board, along with the lead researcher Pamela Michael recast the grant to cover the interaction between the asylum and social conditions in North Wales at the time. Why and when did the communities in North Wales use the Asylum?
They also tacked David Healy on as a medical element to the application. Healy had recently been appointed as a Senior Lecturer in Psychiatry based in North Wales.
The new application succeeded. It led to several papers by Pam Michael and to a wonderful book Care and Treatment of the Mentally Ill in North Wales 1800 – 2000, which brings out the politics of North Wales surrounding the building of the asylum, and the politics of healthcare in North Wales more generally that play similar roles now in 2017 as they did in 1847. The book gives a vivid picture of North Wales life and customs and the way mental illness presented in North Wales settings. This is traditional history well done. (The Table of Contents and Preface for this book has been provided by Cardiff University Press and can be found at the above link).
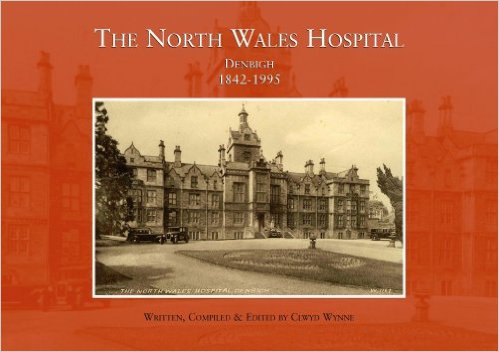
Even before this project had begun a lot of people within the North Wales Hospital were mobilising to preserve some record of the institution. The hospital was scheduled to close in 1995 and one of the senior nursing staff Clwyd Wynne had the brief to collect artefacts and photographs and testimony from both staff and patients about life in the hospital. This lead to the formation of the North Wales Hospital Historical Society and later their website [no longer available at http://northwaleshospital.btck.co.uk/]. It also lead to a book by Clwyd Wynne on the North Wales Hospital Denbigh 1842-1995, with the majority of the photographs featured on this website having been kindly donated by Clwyd.
Historical Epidemiology Emerges
The history embodied in Pam Michaels’ book illustrates the ways in which mental illness presented itself in North Wales 100 years ago. Compared with now it is striking how people for example declared their illness then by escaping from attention through the windows of their houses or by taking their clothes off. This doesn’t happen now. People then didn’t overdose or cut their wrists the way they do now.
Fascinating though this was and is, Healy and colleagues became interested in the quantitative opportunities thrown up by the North Wales Hospital records. Michael’s work involved entering 1 in 10 of all admission records to the asylum. Healy funded the project to enter all records of admissions from North West Wales for the years 1894, 1895 and 1896, with a view to comparing the profile of admissions to admissions to today’s replacement service, the then newly opened District General Hospital, Mental Health Unit, the Hergest Unit, in 1996.
North Wales was made by God for comparisons like this. It is the settling in which Tolkien based Lord of the Rings, with its mountains and castles. The maps of Middle Earth that appear in the Lord of the Rings show the same configuration as North West Wales.
On the left is a map of North Wales, on the right Middle Earth from Lord of the Rings. Tolkien based his story on North Wales geography, with the Hergest Unit based right in the middle of the Shire.
The region is bounded by the sea and mountains on all sides, so that 100 years ago and even now it is not easy to access mental health care from outside the area.
The area was and is poor so that almost all healthcare access was and is through public facilities – there was very little private care.
The area was rural then and remains so today.
It was ethnically homogenous then with 80% of the surnames being traditional Welsh names and is ethnically homogenous now with over 60% still being traditional Welsh surnames.
This meant that with appropriate adjustments for population and control for shifting age bands, from a younger population 100 years ago to the population structure now, it becomes possible to compare the rates at which patients went into the North Wales Hospital 100 years ago and the rates that they enter the Hergest Unit now.
At this point – in September 1998 – Margaret Harris came into the frame. It was becoming clear that the differences between 1896 and 1996 were likely to be striking and that more work would be needed. Harris had majored in history in Bangor University as a mature student and answered an advert for a researcher on the project, a role she filled from 1998 to 2015.
The first striking fact to emerge from the comparison of 1896 and 1996 was that there were far fewer admissions in 1896 compared with 1996. We had to bundle together 3 years’ worth of admissions to make it possible to compare what had been happening then with what happens now.
The second was that the perception that mental health care takes place in small hotel like units now with patients staying for much shorter periods of time and that the care is more effective than before was wrong. We have an enduring image that patients then spent their whole life in the asylum along with over a thousand other inmates in hospitals that had been built to accommodate 100-200 patients at the most but had expanded to hold 1500-2000. This image began to seem wrong.
The third was that the conditions people had were recognisably the same 100 years ago as they are now. Indeed faced with clinical records that contained not just the descriptions of the patient when they came into hospital 100 years ago but also a full record of all later admissions if there were any or the entire course of the patients admission in hospital if they stayed in hospital, it was easier to make diagnosis that several clinicians agreed upon than it is to get agreement on the diagnosis for patients today. Today’s patient on first presentation without the evidence of a clinical course can be far harder to diagnose.
The first article laying out these findings was published in 2001 (see Psychiatric Bed Utilization: 1896 and 1996 compared). To publish it, Harris, Healy and others needed to learn the language of epidemiology and the epidemiologists to whom they turned – Ezra Susser and colleagues in Columbia – had to learn some history.
It was now clear we needed to enter as many records from the past and the present as we could. The records from 1875 to 1924 provided a particular complete group. The Hergest Unit had opened up in 1993. We entered the key demographic and clinical details of all patients entering this Unit between 1994 and 2010.
The ability to make diagnoses and track the course of an illness but also the ability to have a system which gave us a good estimate of the actual number cases each year in a population which remained curiously constant over 100 years then threw up a real surprise – the appearance and disappearance of illnesses.
The first intimation that illnesses might appear and disappear came with the evidence of the disappearance of classic post-partum psychosis. The usual response to this statement is that we still have post-partum psychoses – what are you talking about? There are experts on post-partum psychosis and the profile of this condition remains quite high but in fact the traditional illness has disappeared. Of the cases admitted 100 years ago, 80% were de novo onset in women who had no prior mental health histories and who had not further mental illness once the problem cleared up. It was an intense disorder, with features of delirium. This disorder rarely if ever happens today. The cases we have now are in fact first or further episodes of bipolar disorder that often antedate the post-partum episode which clinically look very different to the cases of post-partum psychoses 100 years ago. And while we were mapping admissions in the modern period, the mother and baby unit in the Hergest Unit, set up for post-partum psychoses closed down. There were no cases. Other mother and baby units across Britain also closed (see Tschinkel et al 2007: Post Partum Psychosis: two cohorts compared, 1875-1924 and 1994-2005).
A second surprise came with our abilities to map the clinical course of Jerusalem syndrome or the schizoaffective or schizophreniform disorders that happen at times of social dislocation. The Welsh Revival in 1904 led to a spike in admissions to the asylum of people with acute and transient psychoses. We were able to track these patients later in life and see what happened. Did they come back into hospital or was the temporary insanity linked to the enthusiasm of the revival against a background of strikes in the North Wales quarries something that was a once off episode? The data made it clear that there were indeed schizophreniform psychoses that have a good outcome.
The biggest beast in all psychiatry, lurking in these and other records, is the question of schizophrenia. The records made clear that for the first 20 years of the period we looked at, the incidence of admissions for schizophrenia was on the rise during the 1875 to 1924 period.
But an equal surprise came in the 1994 to 2010 cohort where admissions began to fall after 2003. This rise in the 19th Century and contemporary fall offers scope to investigate what factors might have appeared during the 19th Century to help make certain psychoses chronic and whether those factors have shown a fall recently that coincides with the drop in the incidence of chronic psychoses. Two factors have been of particular interest to us. One has been the issue of lead contamination and the other has been changes in the nature of obstetrical care during the 19th Century and more recently (see The Incidence of Admissions for Schizophrenia).
At several points during this work over a 20 year period we applied to the Wellcome Trust to fund the work and found that they were reluctant to do so. The contemporary material wasn’t history we were told. When we looked for research funding from epidemiological or other contemporary sources, we heard the historical component was a problem – how can one be certain about events in the past like this.
We ended up creating historical epidemiology – something that hasn’t existed up till this and remains largely unrecognised.
Related to this is the fact that when diseases rise this is wonderful for business and everyone is interested but when they disappear as we found with the post-partum psychoses none of those who have an investment in the disorder are pleased. Our article and our data has fallen on deaf ears even though it has been accompanied by a closure of mother and baby unit across North Wales and elsewhere in the UK. The changes have been as visible as they were with the disappearance of tuberculosis.
In the same way one might have thought that evidence for an increase in the incidence and then a fall in the incidence of schizophrenia would be of wider interest but to date there has been very little interest in this possibility even though there are enormous service implications. Mental health services will need to be reconfigured in their entirety if what we’ve found holds true.
All of the above underpins the reasons for wanting to create this website.
To read more and find out how you can get involved see North Wales & You.
HTV’s desperate letter provided inspiration for young Bangor composer Ellie Davies who has dedicated her most recent work ORDINARY MEN to the servicemen from North Wales who lost their lives in the Great War.[1]
Written in operatic form, the work consists of five movements and when composing the fourth movement – Night Terrors – Ellie looked at the anonymised case notes of some of the soldiers who, as a result of their experiences at the front, were admitted to Denbigh Asylum during or immediately after the war. In her own words, Night Terrors ‘depicts the nightmares of men returned from battle adjusting to life at home’.[2]
Scored for mixed choir and a wind ensemble of flute, oboe and bass clarinet the movement includes snatches of songs which would have been familiar to the men from their childhood in North Wales, the lullaby Suo Gan and a hymn which they are known to have sung in the trenches to boost morale Guide me O thou Great Redeemer.
The voices in Night Terrors have a dual purpose with soloists singing direct quotes from the asylum notes while the chorus expresses the raw delirium of a man trapped within his nightmare. The adapted Suo Gan lullaby is repeated at intervals throughout the movement predominantly by the female voices (soprano and alto) representing the attempts of wives and mothers to soothe their distressed husbands and sons.
The following asylum case note perhaps best sums up the theme of Ellie’s sung libretto:
‘Many who are unable to speak voluntarily yet call out in their dreams expressions they have used in trench warfare and battle’
but she has also incorporated the ‘breaths’ and ‘gasps’ of asylum patients in her work and in fact the work opens with ‘audible breaths in all vocal parts’.
Ellie envisages the case notes being acted out on stage with the intensity of the action emphasised by a flickering light focused on a projection of the empty Eisteddfod chair, Hedd Wyn’s ‘Black Chair’, representing all the empty chairs in all the households that sacrificed a young man to WWI.
The first two movements of ORDINARY MEN – Y Caban and Zero Hour – were performed at the Bangor New Music Festival in March 2016 and the third movement Silent Refrain was workshopped by the BBC National Orchestra of Wales Wind Ensemble in Cardiff in April 2016.
Ellie is hoping that the whole work will be performed next year with the possibility of a recording.
Footnotes
[1] The poet Hedd Wyn’s mother referred to the soldiers who fought alongside her son as ‘ordinary men’ – ordinary men caught up in extraordinary times.
[2] Since graduating from Bangor University with a BMus in 2009 Ellie has worked on a number of community music projects. The performance event Gladstone Fired Up! which she conceived and co-directed originated from a workshop devised by Ellie using her own original music to explore the history of a working pottery museum in Staffordshire. She took a version of this workshop to the Arts and Humanities Research Council’s ‘Connected Communities Festival’ in Cardiff in 2014. Ellie is pleased to be back in Bangor now and looking forward to composing and directing more of the community music she enjoys.
NORTH WALES MENTAL HEALTH RESEARCH PROJECT presents:
Dangerous Asylums
Stories from Denbigh Mental Hospital Told by Leading Welsh Writers:
Glenda Beagan, Carys Bray, A. L. Reynolds, Manon Steffan Ros, Simon Thirsk, Elaine Walker, Gee and David Williams
Contributing editor:
Rob Mimpriss 10th October 2016
£7.95 12.7×20.3 cm 136pp
ISBN-10: 1534608656
ISBN-13: 978-1534608658
A successful London Welshman after the Great War tells his grand-daughter of the madness that infects the family blood. A former inmate at Denbigh Asylum throws herself under a train. A woman made notorious by killing her own child prepares herself for release, and a businesswoman touring a derelict hospital is troubled by the lingering horrors of its past.
When Denbigh Hospital was opened in 1848, it was considered one of the most progressive and humane institutions in Wales, yet it was dogged by over-crowding and rumours of abuse. Now some of the leading writers in Wales tell its story, drawing on the records of patients long dead to give us a portrait of mental illness and care during the Victorian and Edwardian era.
Syphilis appeared in Italy in 1498 just after Columbus had returned from the New World. This later led to suggestions that it had been brought back from the New World, in exchange for the many European illnesses that decimated the populations of North American Indians.
Exposed to a virgin population new infections can be particularly virulent and during the subsequent century in Europe syphilis led to severe physical complications and often death.
A distinctive and horrifying madness
Thereafter its virulence eased, until around 1800 a new and terrible manifestation appeared – general paralysis of the insane (GPI). This was also called tertiary syphilis or dementia paralytica, a distinctive and horrifying madness. Patients cycled through profound depression to extreme elation, psychosis and later dementia before dying.
Stepping back from the illness, doctors could distinguish it from dementia praecox (schizophrenia) by its course – patients cycled through the various stages before dying quite quickly. They were also much more likely to be male. Schizophrenia lasted for decades and was equally male and female. But at any one point in time patients with dementia paralytica and dementia praecox could look identical.
The first recognizable descriptions of both schizophrenia and GPI can be found in an 1809 book on insanity. It took a century to conclusively link GPI to syphilis. The development of the Wasserman reaction which tested for the spirochete, treponema pallidum, that we now know causes syphilis made it clear that this distinctive madness was invariably Wasserman positive. Before that a range of distinctive neurological features made doctors relatively confident in the diagnosis; these included changes to the pupils of the eye and others.
A lifetime with mercury
GPI was a late manifestation of the illness. Syphilis begins with a sore on the penis. For the first most virulent century these sores often extended all over the body – a mark of Cain. But later as the virulence declined they might only appear on the genitals and internal organs. One of the early discoveries was that a mercury salve could help. Administered topically as a paste, the sores sometimes healed. This led to a linkage between mercury and syphilis and the famous phrase of “a night with Venus and a lifetime with Mercury”.
Mercury helped but it didn’t cure. Physicians began to work on methods to get mercury into the body. These included getting the patient to sweat while exposed to mercury vapors, or drinking mercury in the form of Calomel – mercurous chloride. Finally in the 1780s Jacob van Swieten developed a mercuric chloride potion, Van Swieten’s liquor.
Van Swieten was working in Vienna and his brief was the health of the army, whose most serious affliction was syphilis. Soon after his liquor came on the market, the first cases of GPI appear. Could Mercury have caused or contributed to the creation of this mental illness?
No mercury no GPI
Here’s the case against mercury. Many years later in 1925 shortly before he died Emil Kraepelin who coined the term dementia praecox for schizophrenia took a trip to North America to raise funds for his Institute in Munich. One of his interests on this trip was to look at mental illnesses among North American Indians. He was struck by the lack of GPI – even though syphilis had supposedly come from North America.
It also turned out that GPI was rare among American Negroes. A later study in American Negroes infamous for its non-treatment of syphilis, the Tuskegee study, reveals that GPI was much less frequent among American Negroes than among Whites at the time.
Within Europe, Norway offered a striking exception – there were very few cases of GPI. The Norwegians preferred general hygienic measures for managing syphilis and apparently steered clear of Mercury.
Finally GPI was much more common in men than in women, except for one group of women – prostitutes. This seems unsurprising perhaps if syphilis was linked to sex. But if men were infected, their wives were too and should have gone on to GPI also, but didn’t. The initial signs of infection in a woman are more likely to be internal and were accordingly less likely to come to attention and be treated. Women therefore were less likely to take mercury. Except that is for the prostitutes who in a number of cities like Vienna were forcibly treated with mercury in order to reduce transmission.
Against the link to Mercury is the fact that when malarial fever therapy was introduced in 1917, it cured GPI. The conventional view is that the malarial temperatures killed off the spirochete. High fevers of various sorts like this might explain the benign course of syphilis in American Indians for instance.
The Mad Hatter made it clear to Alice
But it is difficult to ignore the role of Mercury if only because the Mad Hatter made it clear to Alice that it can cause psychosis in its own right. Killing the spirochete may have stopped one contribution to psychosis.
This is important for a few reasons. It bears on the story of schizophrenia where a growing case can be made that lead neurotoxicity helped transform some other condition into the chronic psychosis we call schizophrenia.
Pharmacosis – a distinctive and horrifying madness
Unlike lead, which was never used to treat schizophrenia (although there was a surprising amount of lead put into medicines in the 19th century), if Mercury did play a role in GPI, it offers a dramatic example of Pharmacosis – a distinctive and horrifying madness. For much of medicine’s history, doctors were a last resort as their treatments often killed. Hospitals were houses of death rather than cures. But the tally of deaths and injuries in the case of syphilis is particularly poignant.
There is some evidence Mozart contracted syphilis. He knew van Swieten’s son. In the short term mercuric chloride was more likely to cause kidney failure than GPI, which fits the bill for his possible death. Beethoven caught syphilis. Mercuric chloride causes deafness. Schubert caught syphilis and died far earlier than was likely to have happened had he been left untreated. Schumann caught syphilis and is more likely to have had GPI than manic-depressive illness.
In recent years, a bipolar industry has claimed that all great artists have had bipolar disorder – a vanishingly rare and much less common illness in the 1800s than GPI was. It’s much more likely that Van Gogh, Baudelaire, Flaubert and others along with Guy de Maupassant, Friedrich Nietzsche, and Oscar Wilde, had GPI rather than manic-depressive illness.
There is a real case today that many of the antipsychotics or mood stabilizers being given cause the psychoses they are supposed to treat or mood swings they are supposed to stabilize. Misled by a short term benefit, doctors often use these drugs in stupefying doses that eliminate any possibility of recovery – and patients are encouraged to cooperate by being told they are just like Schumann or Van Gogh.
The impetus to this book came in the first instance from Dee Mangin, an academic primary care physician in Christchurch New Zealand, who drew the attention of one of us to a famous quote from Pinel: “It is an art of no little importance to administer medicines properly: but it is an art of much greater and more difficult acquisition to know when to suspend or altogether to omit them”[1].
Chasing the context of this quote further made it clear that this came from Pinel’s 1800 Treatise on Mental Alienation, and that his 1809 Treatise, his definitive work, had never been translated into English. Not only that but the translation of the 1800 Treatise was likely the worst translation of all time of any major work.[2]
The 1809 Treatise is a landmark work in the study of the mind. In these pages Pinel can be seen grappling with the enduring issues of insanity and their intersection with his time. He had to accommodate on the one hand contributions on the issue of insanity stretching back to the Greeks, while at the same time disengaging from the claims of other authorities such as the Church when it came for instance to dealing with pathological piety or religious delusions, and he had to negotiate these issues at a time of unparalleled social upheaval.
The tensions come through dramatically at points where he outlines clinical interventions to destroy religious materials he suspects have aggravated the condition of his patient, and where he blames misguided spiritual advice for leading to relapses. They also come through at points where he insists that remarkably different mental abilities may be differentially affected by illness; the reader may wonder why Pinel insists on what is for us so unremarkable but in fact these observations that seem so mundane posed a profound threat to the doctrine of the unity of the soul.
This was a point in history where longstanding domains of influence were being reconfigured[3]. Where once authorities such as the Church and traditions that stemmed from the ancients were unchallengeable, Pinel’s generation hoped that the science of ideas (as we have translated ideologie) might triumph and lead to progress of the kind produced within the physical and biological sciences[4]. As a prerequisite of such a science, it was necessary to cast aside tradition and observe patients.
The emerging asylums gave him an opportunity to chart the course of his patients’ disorders, and he described their situations and their problems with a vividness not seen since Hippocrates, and charted the course of their disorders in a way that had never been done before. He was the first to introduce the dimension of time into the consideration of mental illness, most evidently in his new notion of folie périodique, which helped lay the basis for the clinical approach to mental illness that flowered with Kahlbaum and Kraepelin, giving rise to our concepts of dementia praecox and manic-depressive illness.
Pinel hung his argument on these clinical descriptions, in a manner that is truly modern. While his classification of disorders may take some getting used to for modern readers, he outlines a range of clinical phenomena that readers will readily recognise – such as the role of expressed emotion in aggravating conditions, the concepts of relapse and relapse prevention, notions of an iatrogenic overlay on a primary condition, and problems that stem from polypharmacy – actually employing the term polypharmacie (para 279).
Philippe Pinel 1745-1826
For those interested in historical antecedents to modern notions, this is the text to cite not only for the origins of these psychiatric notions, but also the first text to advocate clinical trials, as well as a recourse to probabilities and statistics to assess the efficacy of a treatment, and the first to call for an evidence based medicine.
When one gets used to the words being used, the classification Pinel suggests is in fact less alien than many might suspect, in that he distinguishes between shifting or multipolar states and conditions which show invariance or unipolarity in a manner that anticipates later 20th century thinking on unipolar and bipolar dichotomies[5]. In outlining these ideas he gives new meanings to the terms mania (“manie”) and melancholia (“mélancolie”) that had previously referred essentially to overactive and underactive insanity.
Of all the terms in the book we have struggled with none more than with manie. Mania was the equivalent English term of the time, but mania then and mania now are two completely different things. Over half of the patients admitted to a facility for the mentally ill from Pinel’s day through to 1900 had mania. Patients, who would now be diagnosed as having schizophrenia or agitated depression, were diagnosed as having manie. Emil Kraepelin’s creation of dementia praecox and manic-depressive in 1896 led to the demise of this form of mania, and the diagnosis shrank rapidly in frequency thereafter[6].
Manic-depressive illness remained a rare disorder for a century but in recent years we have succumbed to a “mania” for bipolar disorder that is leading all sorts of patients to be diagnosed as having manic episodes who until 10 years ago would never have been diagnosed in this way, including overactive infants. A mania diagnosis now leads on to treatment with mood-stabilizing drugs. Even the briefest reading of Pinel’s Treatise will make it clear he would never have condoned this.
There is in brief almost no commonality of meaning between Pinel’s manie and this 21st century mania and so we have struggled to find the right term for manie. Initially we translated it as insanity. There was one big disadvantage to this approach which is that it conceals Pinel’s realisation that ‘manie’ was one of the species of madness rather than the primary genus of mental alienation. This realization led him to a change in title between the first edition of the Treatise entitled, “Traité médico-philosophique sur l’aliénation mentale ou la manie,“ and the second edition entitled “Traité médico-philosophique sur l’aliénation mentale’.
Following input from Dora Weiner, Professor of Medical Humanities and History at UCLA, we finally settled on maniacal insanity, having rejected manic insanity en route as manic is too closely linked to the modern usage of mania. Maniacal in contrast paints a picture of overactivity, disorganisation and agitation that appeared to fit the bill quite well.
This brought us to mélancolie. Pinel’s new definition of melancholia focussed attention on the single delusional system that these patients typically had. This brought his melancholia quite close to the form of disorder that attracted this diagnosis for the greater part of the 20th century. On this basis we opted to hold on to melancholia.
One of the problems both Pinel had as a clinician, and we as translators have had, is that term delusion was not available to him. Mad patients with what would now be called delusions were then termed delirious (délirants). This led him to coin terms like exclusive or selective delirium (‘délire exclusif’). In translating the text we have grappled with issues like this and used delusion rather than delirium where indicated. The problem is that the French word “délire” does not clearly distinguish between the states referred to by the English terms “delusion” and “delirium”.[7]
Combining these difficulties, Pinel also famously introduced the concept of ‘manie sans délire’ to designate ‘moral’, ‘emotional’ or affective insanity, a notion easily confused with, and invariably mistakenly associated with psychopathy.[8] Reading the treatise however makes it clear that Pinel was distinguishing these states from ‘cognitive’ insanity characterised by delusions and that he had in mind a range of conditions without frank delusions or confusion that would for the most part today be categorised as mood disorders, or obsessive compulsive or other disorders. We have opted to translate this as insanity without delusions.
He illustrated the new disorder in a number of vivid vignettes, none better than his description of what happened when the Bicêtre was stormed by revolutionaries expecting to find and hoping to liberate many who had been inappropriately incarcerated (para 161). Thinking they had found one such individual, on the basis that he did not appear to have frank delusional ideas, they swept him off triumphantly, only to return him a short while later conceding that he was indeed mad. In the case of this and other concepts such as ‘folie raisonnante’, the quintessential French antecedent of the modern delusional disorder, we have translated the concept but retained the original French term also.
Pinel also uses dementia and idiocy as classificatory terms but many readers will suspect from the descriptions he gives that included among the dementias, and even among those with acquired idiocy, are some patients with dementia praecox.
We have also had to grapple with words like ‘chagrin’. Key to Pinel’s thinking was the possibility that the passions, of which chagrin is the most commonly mentioned, might give rise to insanity. This word was also common in English in 1809 and referred to a powerful affective state. But the word is rarely used in Britain now, while in America it is commonly used but refers to an inconvenient embarrassment rather than the kind of re-sentiment that might lead to madness. We have opted to translate it for the most part as chagrin, and sometimes as deep sorrow. The use of lost concepts like chagrin and misanthropy which once featured prominently in our efforts to understand ourselves, might hopefully act as a reminder that there have been other ways to see some of the issues at stake. Looking back can sometimes make visible the way forward – reculer pour mieux sauter.
While advocating an awareness of the passions as triggers to insanity, Pinel holds in conjunction all possible triggers to the conditions his patients evince, noting the physical changes in bodily functioning which he argues may lead on to secondary mental changes, and then outlining case histories in which events and circumstances that lead to powerful passions such as chagrin or anger trigger identical mental disorders to those that seem to have physical antecedents. This is an aetiological account that to this day still elicits support from all sides of psychiatry’s divides.
But he pierces to the heart of psychiatry’s divides in the treatment domain. First and famously he advocates moral treatment. As translators we have had to struggle with this term[9]. While it is often translated as psychological treatment, and the word psychology had been in existence from 1682, the idea of a psychotherapy did not come into existence before Freud and Janet almost a century later, and using a term like psychological treatment risks importing ideas into the mix that were just not available to Pinel. The term behaviour therapy maps well onto what he actually did, and behaviour therapists now cite him as the originator of their discipline[10], but equally this is a 20th century term that risks misleading. There are also ethical senses of the term moral that need to be carefully noted and held at arms’ length.[11]
Painting by Tony Robert-Fleury (1876) ‘Pinel a la Salpêtrière (1795)’ – Dr Pinel ordering the removal of chains in the Paris Asylum for Insane Women.
We have opted in most instances for mental treatment as a way forward. This is a concept that can accommodate psychodynamic, behavioural and other possibilities. It opens a space for clinical wisdom of the type Pinel approves when he refers to Galen’s diagnosis and treatment of a women in love – outlined in footnote 3 in his introduction. There are at least three versions of this story in ancient medicine, of which the best known may be the Stratonica story. In this version, Seleucus, the King of Syria, then in his sixties is given the young Stratonica in marriage. His son Antiochus falls in love with her and wastes away, until the King’s physician makes the diagnosis on the basis of changes in the youths pulse whenever she is near[12]. Pinel makes clear his approval of clinical skill of this kind and his book is an attempt to build on this approach.
Finally he also advocates the use of a new institution purpose built to treat the mentally ill – one that he refers to as a hospice, which his pupil Esquirol later called an asylum. This would differ from the facilities in which the mad were previously confined in that patients would be separated according to the state of their disorder, would have their treatment plans tailored to their state, and where they might not only have their wits restored but where they might have had the opportunity to consolidate their recovery.
At a time when the height of fashion is to advocate treatment at home and to avoid admission to any kind of facility, Pinel offers a persuasive case against home treatment (See para 229 – 231, 275 – 276, 309, 352, 364, 395). He is confident in the capacities of an enlightened institution, with responsible people at its head, to improve the lot of the afflicted. He contrasts such an institution with the kinds of facilities previously available, such as the Hotel Dieu, where patients were likely to be brutalised by unsupervised care staff and debilitated by the treatment and procedures advocated by medical staff.
Pinel’s hospice is a far cry from the total institutions that Erving Goffman in his book Asylums, 150 years later, claimed created the clinical pictures that mental health staff categorised as illnesses[13]. It was a facility where recoveries were consolidated through work, and this example led on to the tradition of asylum farms and sewing rooms. Today we are apparently rediscovering the values of rebranded ecotherapy and ergotherapy, but it seems following Goffman’s total stigmatization of the Asylum recovering the notion of an asylum is just not possible.
In part, we have stuck with Pinel’s designation of the mental health facility within the Salpêtrière as a hospice as the word asylum was not available to him. But in part we have also opted for hospice rather than asylum, as the latter has been so stigmatised in our day that another word is needed to convey the benefits that enlightened institutional care might offer. To deny any possible benefits is fashionable but in a wider frame of reference risks looking more like a romantic denial of illness itself.
This book can be read on many different levels. On one level there are a series of human dramas Pinel so deftly sketches. He is first and foremost a clinician – one of the first modern clinicians, as Dora Weiner brings out in her preface to this volume and in her biography of Pinel[14]. On another level there is his articulation of the merits of the public domain, and its institutions, guided by the latest science. This is not just a matter of public versus private monies but rather as he makes clear a matter of the progress that can be expected when competing interests are brought to the light of day – a public morality that will be built on the progress of science.
In our own day confidence in public science is low. There is it seems a greater confidence in business and market solutions. But on this point Pinel throws down a challenge to the marketplace. Physical and mental treatments can all be marketed, as can a humane and decent delivery of these treatments, but the market cannot readily handle ‘No’. The market comes with a bias toward action and doing, ever giving another treatment if the first fails, or combining treatments in ever more elaborate cocktails. But there is here a fundamental retreat from wisdom, as the 1800 quote cited above illustrates. This quote is not repeated verbatim in the 1809 Treatise, but its thrust comes through repeatedly in the text. While Pinel advocates evaluating treatment, his treatment approach is ultimately underpinned by wisdom, a wisdom that may sometimes simply mean interfering as little as possible with the healing powers of nature – a central premise of his ‘médicine expectante’ (para 157). This was a wisdom that seemed to him more secure in the public domain.
David Healy, Louis C Charland, Gordon Hickish
The full translation of Pinel’s Treatise on Mental Alienation is available for free here or directly from Wiley’s online Library.
Acknowledgements: We have worked from the recent French reissue of the 1809 Traité:
Pinel P. Traité médico-philosophique sur l’aliénation mentale. Paris Seuil, 2005.
We gratefully acknowledge a huge input with key French words and passages from Dora Weiner, who co-edited the recent edition of the 1809 Traité with Jean Garrabé.
We had further input on concepts and practices from Monique Debauche, and Philippe Pignarre, the publisher of the 2005 edition. Marilyn Gower helped us to translate sentences from Latin.
[1] Mangin D, Sweeney K, Heath I. Preventive health care in elderly people needs rethinking. BMJ 2007, 335, 285-287.
[2] Weiner Dora B (2000). Betrayal! The 1806 Translation of Pinel’s Traité médico-philosophique sur l’aliénation mentale, ou la manie. Generus 57: 42-50.
[3] Weiner Dora B (2002). The Citizen-Patient in Revolutionary and Imperial Paris. Johns Hopkins University Press, Baltimore.
[4] “Ideologie” stemmed from the ideas of Cabanis, Destutt de Tracy, and others who, following Locke, believed that ideas in the environment could change people’s thoughts and behaviour, and as such needed controlling ideally by a scientific approach.
[5] Healy D. Mania. Johns Hopkins University Press, Baltimore 2008
[7] Berrios, G.E. A History of Mental Symptoms. Cambridge: Cambridge University Press, 1996.
[8] Berrios G.E.. Introduction to ‘J.C. Prichard and the Concept of Moral Insanity’. Classic Text No. 37. 1999; 10: 111-116. See also, Shorter, E.. A Historical Dictionary of Psychiatry. Oxford: Oxford University Press, 2005, pp. 213, 239-240.
[9] King, Lester S. A note on so-called “moral treatment.” Journal of the History of Medicine, July 1964, 297-298.
[10] Marks I. Marketing the Evidence. In Healy D, The Psychopharmacologists II, Arnold, London, 1998, p 543-560.
[11] Charland, L.C. Benevolent Therapy: Moral Treatment at the York Retreat. History of Psychiatry, 2007, 18(1): 61–80.
In 1889 American born, Florence Maybrick at the age of just 27 was charged with the murder of her husband following his death in their home town in Liverpool. She was subsequently convicted and sentenced to death.
Her case attraction considerable attention with extensive newspaper coverage both across the UK and also in the United States.
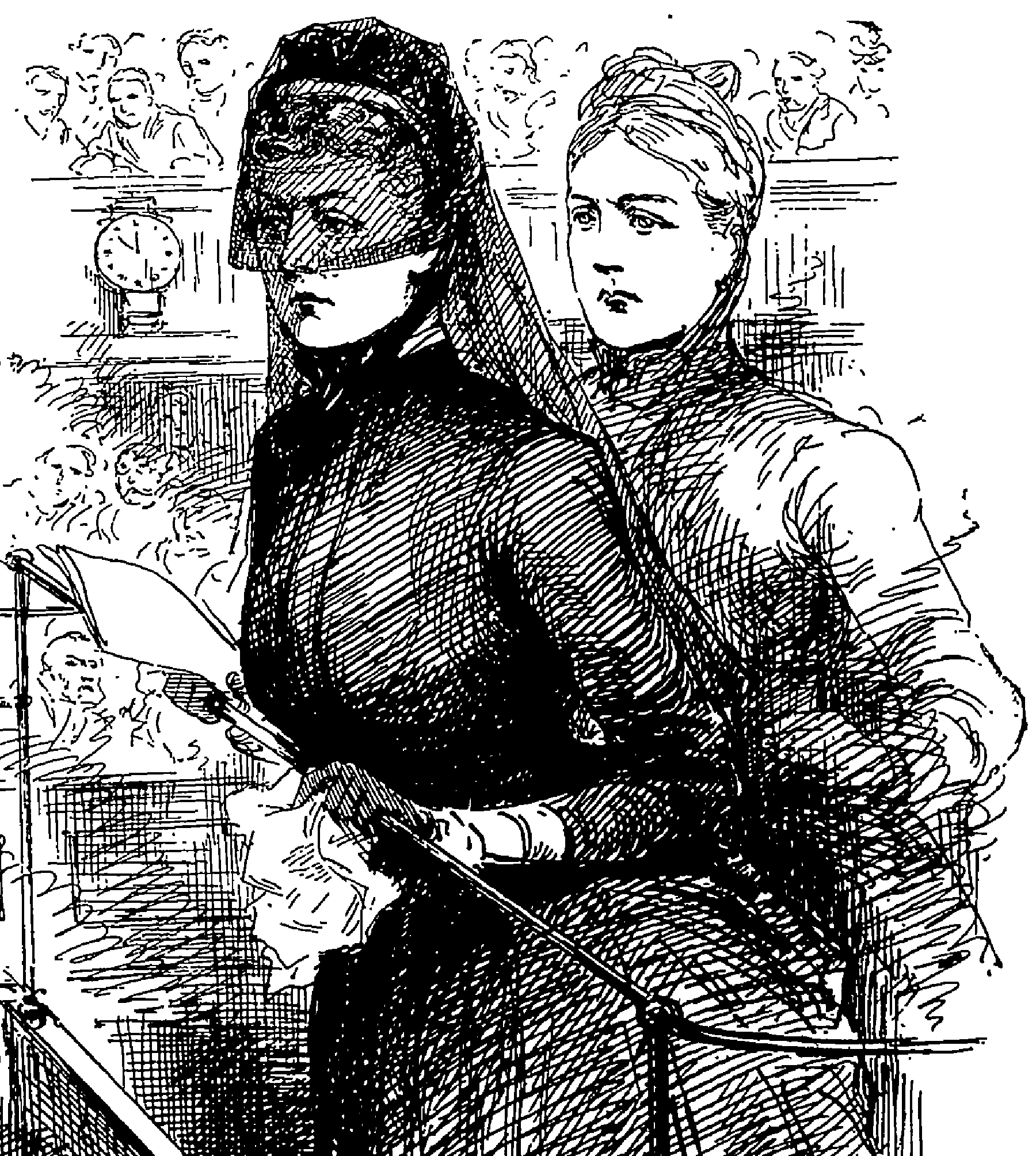
Reports in The Penny Illustrated included drawings of the ‘exceedingly comely and graceful’ Florence Maybrick in full veil reading her statement from the dock.[1] There were also pictures of the family home, of the late James Maybrick, the Maybrick children, Mr Brierley, the trial lawyers and Judge Stephen. It all made for a good read!
A few voices were raised in support of the verdict against Mrs Maybrick but these were drowned out by the voices of those who believed she was being condemned on the basis of her immorality – she was said to have had an affair with another Liverpool businessman, Mr Alfred Brierley, and to have booked into a London hotel with him – rather than on any firm evidence that she had set out to murder her abusive, hypochondriacal and much older husband James.
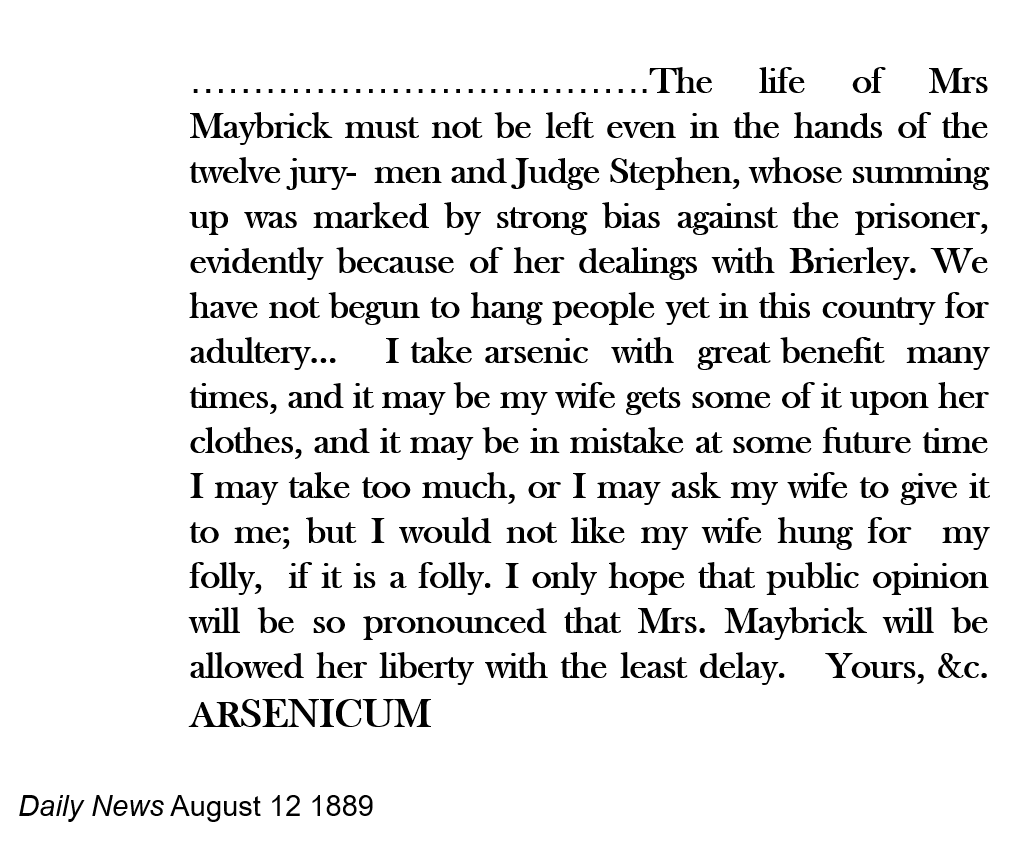
Letters questioning the legal strength of the case against Florence Maybrick dominated national and local newspapers. And ‘ARSENICUM’ raised the possibility that other women could place themselves at risk of being accused of murder simply by miscalculating the dose of what was then considered a perfectly legitimate tonic or even by wearing contaminated clothing.
Following this public outcry and in response to mass meetings and petitions demanding a reprieve, she was saved from the gallows at the last hour – the workmen had already started building the scaffold.
Her death sentence was changed to that of a life sentence and Mrs Maybrick spent 14 years in prison. On her release she returned to America, where she went on to live a reclusive life in Connecticut, tragically never seeing her children again. She died alone and destitute in 1941.
According to reports among the very few possessions she left behind was a tattered old bible in which, tucked between its pages, were directions for soaking flypapers for use as a beauty treatment.
There is something of the divided mind even in the naming of this landscape. Its indigenous tribes were called weallas – foreigners – by Saxon sailors and invaders, and thus the country gained its English name: Wales. But to those native people themselves – Y Cymry, “our people!” – it was Cymru. The mountains of the north were not Snowdonia (from the Saxon Snawdune) but rather Eryri, which is traditionally and maybe inaccurately translated as “haunt of eagles”.
What of its character, and the interplay between physical land-forms and human history and personality? There’s a wonderfully sonorous and resonant line by the twentieth-century poet from Bala, Alan Llwyd. It runs thus:
Bywyd gwar mewn byd gerwin
And it translates roughly as “a civilized life in a rough world”.
Throughout the first millennium of this region’s written history, the abiding impression is one of a minority civilization inhabiting here under threat from barbarism and invasion. I’d hazard that Welsh traditional culture, clinging to the language which is its means of expression, still feels itself thus in jeopardy, through the swarming influx of recreationalists and second-home-owners; who know nothing and care less of what native riches may here be found; who never bestow a moment’s attention on this region’s human character.
Six centuries of military conquest and subjection, followed by a further three in which an initial trickle of tourists turned into the contemporary deluge, are likely to have bred degrees of resentment. Local populations cannot view those masterpieces of military architecture to be seen at Caernarfon, Harlech, Conwy with quite such appreciative interest and satisfaction as the world-heritage-site aficionados who flock to visit them every year. To a native mind their presences still carry oppressive symbolic weight.
We must balance this with what external consciousness brought by way of appreciation for the mountain landscape, with its exquisite valleys, its oakwoods and birdlife, its high rocky ridges and shapely summit crests.
Historical circumstance played a crucial role here. Edmund Burke’s seminal 1757 essay in aesthetics, “A Philosophical Enquiry into the Origin of Our Ideas of the Sublime and Beautiful”, had scarcely been assimilated into educated English consciousness before the French Revolution and its aftermath placed the most sublime of European landscapes – the Alps – off-limits. The mountains of North Wales filled the breach and a generation of Romantic celebrants – Richard Wilson, William Wordsworth, J.M.W. Turner – fixed them in the cultural imagination.
All this fed back into a Welsh consciousness that had in recent centuries perceived its home place either through the beauty-shunning lens of Calvinism, or as a working landscape: of sheep-farms and slate-quarries, of flannel-mills and copper-mines. The hills became a place of resort for artists, poets, writers. Later came the mountaineers, and their sub-sect of rock-climbers, among whom in the 1930s was the tragic figure of Menlove Edwards, a psychiatrist and the finest and most original of all writers on his sport.
Now it is a place of recreational resort to which huge numbers are drawn to pursue what those of the tight-knit valley-communities, the run-down slate-towns and the forlorn coastal settlements might consider in their essence to be neo-colonial. Native knowledge is ignored or traduced; not one in a hundred of casual visitors to these mountains gives any more than at best a token respect to the language in which their characters, histories, namings are expressed.
So resentments simmer. Misunderstandings too. A population feels itself devalued. If the colonization itself is scarcely done by stealth, its effect in the extirpation of a topographically-rooted culture and a way of life and means of expression shaped by hill-forms that have at times a formal beauty something akin to musical notation is less strident but as insidiously effective. Rifts widen, anger grows, human equilibria are thus destabilized.
Those peaks, those plunging valleys – they have their counterparts, their objective correlatives, in the jagged landscapes of dispossession, disregard and the suffering mind.
This website details some of these patterns and histories of response. It seeks more, and not less, understanding; studies cause and effect; sees the skull beneath the skin of a landscape as beautiful as any in Europe; is a vital adjunct in the study of this place and the history of mind that inhabits here.
Back to that trope about the foreign, and by implication the alien and the excluded, with which we began. No-one’s thus on this website. You’re all our people – come on in, enter the ‘region of summer stars’ as the sixth-century poet Taliesin called Wales, and see what we have to offer each other.
The solution Dr Orange came up with to deal with the problem of communicating with Catherine Jones was to employ a South Walian woman ‘with a knowledge of the Welsh language’ to translate.
However, there was someone else in Broadmoor at the time that he could have called upon – Mary Davies from Llanfaelog, Anglesey. But while Mary probably had more than a mere ‘knowledge’ of Welsh she may have been considered unsuitable to deal with a comfortably married, respectable farmer’s wife whose physical condition was precarious.
A prostitute of ‘generally bad character’, Mary already had three earlier convictions for larceny when she was tried at Beaumaris in 1873 at the age of 18. At that point she was not thought to be insane and was sentenced to 7 years penal servitude at Millbank Prison (now the site of Tate Modern) followed by a year of police supervision. Her prison occupation was knitting. When a series of medical observations at Millbank and later Woking confirmed her insanity, she was transferred to Broadmoor with personal property valued at £6.1s 6d.
It may have been Mary’s bad behaviour at Broadmoor – she is recorded as violent and liable to strike out – that persuaded Dr Orange she would not be a suitable companion for the rather frail Catherine. Or it may have been that, as a prostitute and convicted felon, she was thought morally unfit. Either way, there is no indication she ever met Catherine Jones in Broadmoor and by the time Mary was transferred to Denbigh in 1880, described as ‘demented and incoherent with mania and can attack sometimes at the catamenial periods’, Catherine had already returned to her family in Llanllyfni.
Nicknamed ‘Broadmoor’ by the Denbigh staff, Mary Davies was ‘occasionally passionate’ but she proved useful in the kitchen and remained in the asylum until her death in April 1914 from heart disease.
“What is the most desirable situation for an hospital for the insane?
We may presume, without further question, that the same circumstances, in regard to situation, which are found by a person who is free from any morbid tendency, to have a beneficial influence on his mental feelings, will generally, in some degree, contribute to the restoration of a mind diseased.
The establishment should be situated, then, under a mild sky, in an agreeable, fertile, and sufficiently dry part of the country, where the surrounding scenery, diversified with mountains, valleys, and plains, is calculated to enliven the spirits of the beholder…there should be an unfailing spring of good drinking water…and easy communication with some large market town.”[1]
The location of the North Wales Lunatic Asylum, opened in 1848 to serve the five counties of North Wales, almost perfectly realised Jacobi’s vision. Nestling amongst the rolling hills which mark a border between the fertile Vale of Clwyd to the east and the rugged Hiraethog moors and Snowdonia to the west it also lay within easy walking distance of the thriving agricultural market town of Denbigh which, by the 1860s, was to become the main centre of the Vale with rail connections to London, the Midlands and the North West.
In the autumn of 1874 Dr George Turner Jones, who had been Medical Superintendent of the asylum since its opening, was terminally ill. He had supervised the care of more than 2700 patients during his 26 years in post and it seems he had adhered as closely as possible to the philosophy of humane treatment for the insane which underpinned the 19th century asylum building programme.
Dr Jones would have employed the limited medications available to him, along with wine and brandy, as part of a therapeutic regime. However, in 1869, he was keen to investigate the curative properties of the Turkish bath and made arrangements to visit asylums at Cork and Limerick where baths had been installed and were apparently effective, with Dr Thomas Power claiming that half of his patients at Cork were improved or cured after using the bath.[2]
After this visit to Ireland, Dr Jones strengthened his recommendation for a Turkish bath at Denbigh by adding that “as a means of cleansing it is found to be the cheapest mode adopted” and the Committee of Visitors approved its immediate construction.[3]
The Lancet had insisted in 1861 that the medical properties of the Turkish bath were unknown and denounced the literature on the subject as “for the most part, either puffs or long descriptions of baths, ancient and modern, with a few instances of cures affected”. The journal had called for “a fair and scientific trial” to be made at a metropolitan hospital under the direction of medical officers.[4] It appears that no such trial had been conducted by the time the Committee of Visitors at Denbigh made their decision because Dr Jones was condemned in 1870 for making an extravagant claim as to the percentage of cases cured by the Turkish bath and failing to produce any exact statement of its real scientific value.
In a letter to the Lancet in February 1871, Dr Edgar Sheppard, Medical Superintendent at Hanwell Asylum (the only asylum in England to have a Turkish bath at this point), wrote in defence of Dr Jones. While agreeing that his statement regarding cures was probably an error, he argued that:
“It is probable that… 74 per cent of “recovered” cases had been treated by the Turkish bath with markedly good effect, rather than that 74 per cent of insane cases had been absolutely cured by it.”
And in criticising the Lancet for insulting medical superintendents generally:
“We can afford to bear, and smile at the abuse. We may not be doing much for what you and others call science, but we may still be labouring hard, and not unsuccessfully, to bring about the cure and well-being of our patients”.[5]
In 1871, in the midst of these professional disagreements, the asylum at Denbigh became the fourth asylum in Britain to install a Turkish bath and Dr Jones was soon reporting a marked beneficial effect in several cases of acute mania, adding that: “I am fully persuaded of the superiority over the ordinary warm bath in its cleansing power. The peculiarly disagreeable odour which is emitted from the secretion in the skin of the insane is perceptibly modified by the Turkish bath”.[6] The association of insanity with a particular smell appears to have been widely accepted in the 19th century and is discussed in medical journals of the period. An article in the London Lancet of 1830 describes the “maniacal odour” as “a pathognomonic symptom so unerring, that if I detected it in any person I should not hesitate to pronounce him insane, even though I had no other proof of it”. [7]
Regardless of this, patients also approved the Turkish bath – it was much less objected to than the ordinary warm bath water – and the Commissioners in Lunacy observed in 1872 that they used it generally instead of the baths in the wards.[8] By 1874 the average number of patients taking the bath weekly amounted to 170 men and 180 women representing about 85 per cent of the inmates.[9]
Dr Sheppard’s robust response to the Lancet’s criticisms of the scientific shortcomings of medical superintendents – that their work was more focused on the wellbeing of their patients than on research – is borne out in the records from the North Wales Lunatic Asylum during this period.
While the therapeutic value of a limited drugs armoury and Turkish baths remained unclear, the need to provide meaningful employment for patients and opportunities for recreation was never questioned. Male patients worked on the asylum farm or in the garden. Skilled craftsmen were able to work with the joiner, tailor, shoemaker, blacksmith, painter or butcher and some of the better educated patients assisted the steward or clerk with clerical duties. Female patients knitted or sewed, others worked in the laundry or kitchen or on the wards. All patients capable of occupation were employed in some way.
Weekly dances had been introduced in 1864 which, apart from being enjoyed by patients, provided a useful opportunity for the medical staff to observe behaviours. Around 220 patients of both sexes regularly danced to music from the asylum band and in the summer there were dances on the bowling green. Case notes suggest that a patient’s conduct at the weekly dance could be taken to signify the likelihood of recovery or relapse. Elizabeth Phelps Gapper, a young governess employed at Dolgelley, was admitted onto the refactory ward with acute mania but after a few weeks was permitted to attend the dances and once it had been observed that ‘she conducts herself in an orderly manner’ she was soon discharged.[10] There were concerts, ‘private theatricals’, a brass band and in 1873 it was reported that:
“Every object for the amusement of the patients has been resorted to. Several dramatic performances and amusements were attended by many of the most excitable patients and their conduct has been so encouraging that in future we hope to extend these entertainments”.[11]
The asylum was surely a cold, uncomfortable place with its stone floors and poorly lit corridors but the vast majority of its patients were paupers whose lives outside the institution may have offered no greater physical comfort and in some cases a great deal less. Not infrequently, patients admitted in a malnourished condition left the asylum ‘quite stout’ and there are examples of recovered patients who asked to be kept a little longer, like WO who, on his second admission, did not want to miss the Christmas celebrations he had enjoyed the previous year.[12]
Christmas festivities were a highlight of the year when patients helped staff to decorate the asylum in preparation for an annual feast of roast beef and plum pudding. “On Christmas Day, over a hundred of each sex sat down together in the large room to their annual feast” when “the cheering and soothing effects of occasionally mingling the sexes are very observable.”[13]
Prior to being discharged, all patients were required to appear before the Committee of Visitors where they would be questioned as to the treatment they had received in the asylum. The Committee reported in 1873 that: “In every instance the patients have expressed their gratitude for the considerate manner in which they have been cared for”.[14]
Dr Jones’ deteriorating health forced him to resign in October 1874 and he died the following year. Dr William Williams, assistant medical officer at Hanwell Asylum under Dr Edgar Sheppard, was appointed his successor but until he was able to take up his post on 1st January 1875, Dr Evan Powell served as acting medical officer in charge.
It was therefore Dr Powell who presented the medical superintendent’s annual report for 1874 and it is clear from this that cracks were beginning to appear in the system. He described patients admitted during the year as being “of a most unfavourable class on account of their advanced ages, bodily infirmities and the form of their mental diseases” and regretted that so many chronic and imbecile patients were being sent to the asylum.[15] This Dr Powell attributed to a government subsidy which made it cheaper for Poor Law Unions to maintain paupers in the asylum rather than in the workhouse:
“The crowded state of the asylum, especially on the female side, will very shortly become an important subject for the consideration of the committee. We would recommend as a temporary remedy the removal of the chronic and harmless patients to the workhouses.”[16]
Dr Powell also expressed his disappointment that, because family members had objected, so few post mortems had been carried out during the year. “It would be very desirable if a rule could be established by which a post mortem examination could be made in every case.”[17]
Dr Powell’s frustration was shared by his successors and the need for more post mortem examinations is frequently mentioned in subsequent annual reports. There are hints of a progressive approach to medicine in Dr Powell’s diagnoses. In earlier reports these fell into four basic categories – mania (acute, puerperal and chronic), melancholia, dementia, epilepsy and idiocy. But in Dr Powell’s report mania could also be recurrent, melancholia could be acute or chronic and idiocy had a sub group ‘with epilepsy’. Kleptomania appeared on his list, also monomania with and without suspicion, and delirium tremens. Dr Powell left his post at the asylum[18] soon after delivering his report and diagnoses generally returned to the more conservative groupings of previous years.
In January 1875, when Dr Williams took up his post at Denbigh, the asylum was almost full, with a large proportion of beds occupied by chronic long stay patients who had been accumulating year upon year since the asylum’s opening. The need to make provision for curable cases of insanity demanded that the problem of providing alternative accommodation for these long term chronic cases be addressed. It was a problem which would dominate Dr Williams’ time at the North Wales Lunatic Asylum and become an even more pressing problem for his successors.
Footnotes
[1] Jacobi CWM (1841) On the Construction and Management of Hospitals for the Insane.
[2] Kandela, Peter (2001), The rise and fall of the Turkish bath in Victorian England, International Journal of Dermatology, Vol 39, Issue 1.